
INTRODUCTION
Definition and etiology
Shoulder dystocia is an unpredictable obstetric emergency1-12 and is related with neonatal morbidity and mortality and in some severe cases with maternal complications1,4,13-18. It is defined as a vaginal birth that requires special maneuvers after the neonate’s head has been delivered and the birth of the fetal shoulders has failed2,19. Shoulder dystocia complicates approximately 0.5– 1% of vaginal births1-3,13,19,20. Nowadays, this percentage is increasing because there are bigger neonates being born than in the past and possibly due to the increased use of epidural anesthesia. Furthermore, the percentages may be different depending on the size of the fetus. Specifically, the likelihood for shoulder dystocia is about 1% for fetuses weighing <4 kg, 5% for fetuses 4–4.5 kg, and about 10% for fetuses weighing >4.5 kg18.
Risk factors
Macrosomia of the fetus is the most significant risk factor for shoulder dystocia2,4,6,13,15,19,21-23, however other risk factors are also responsible, for example: maternal diabetes2,4,6,19,21,24, previous history of shoulder dystocia2,6,19,20,25, pelvic stenosis, large maternal weight gain20,26 or maternal obesity2,6,19,20, male gender, multiparity, assisted vaginal delivery with vacuum or forceps, prolonged second stage, and >42 weeks of pregnancy etc. Only 50–70% of the risk factors can predict shoulder dystocia, except of gestational diabetes2,19. Moreover, despite fetal macrosomia being the most significant factor for shoulder dystocia, >50% of the cases occur in pregnancies with a normal birth weight fetus.
Shoulder dystocia should be differentiated from breech delivery and umbilical cord prolapse and ‘delay of shoulder delivery with normal head rotation’27.
Complications
Shoulder dystocia is associated with a variety of complications for the fetus such as: paresis of brachial plexus2,4,11,15,16,19,20,28-31, perinatal asphyxia2,11,16,19,30,31, hypoxic-ischemic encephalopathy2,19, humerus fracture27, clavicular fracture2,11,15,19,31, and perinatal mortality2,19,30. Furthermore, soft tissue injuries are the most common maternal complication, with an increased rate of third- and fourth-degree lacerations or tears in the vagina and vulva.
CLINICAL MANAGEMENT
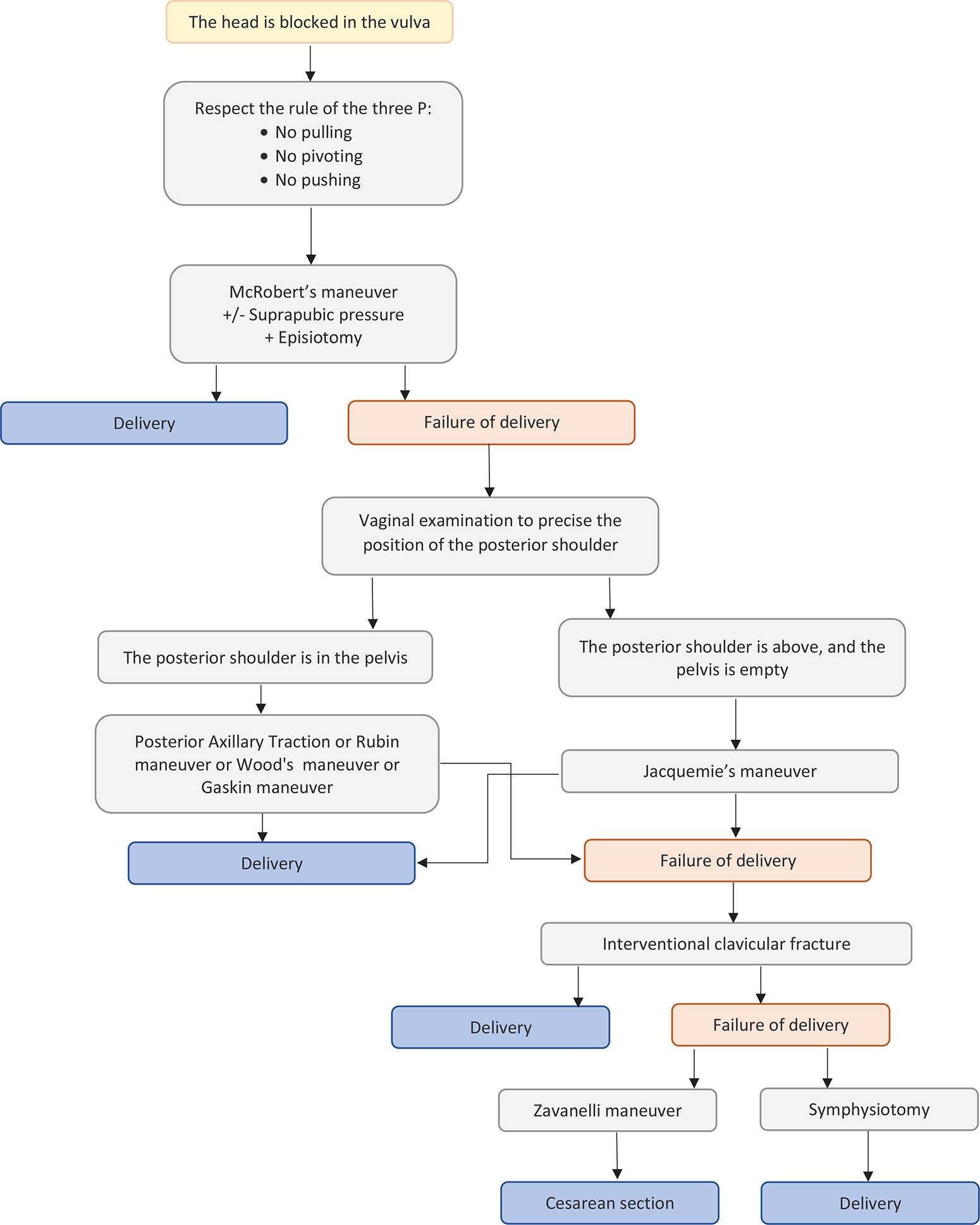
Midwives and obstetricians should be able to deal with shoulder dystocia at any time6,10,32. This means that they are adequately and distinctly trained1 through simulation3,4,33 so that they know how to perform obstetric maneuvers2,5,10,19 and apply the protocols1,3,5. The main aim is to reduce the birth interval between the head and body in order to reduce the risk of birth asphyxia and to deliver the neonate without damaging the brachial plexus by pulling the neck7. When shoulder dystocia has appeared, it is of great importance that the physician recognizes the situation and immediately asks for help from other team members. All the known maneuvers are typically divided into simple and complicate maneuvers that are described below. It is noteworthy that the recommendation about the appropriate amount of time to spend on each maneuver is up to 30 seconds. Figure 1 describes the algorithms for the management of shoulder dystocia.
First-line maneuvers
McRoberts’ maneuver
This maneuver was introduced in 198334. It is a simple but effective maneuver35,36 of vaginal delivery where the patient is in a lithotomy position with abducted legs bending the knees at the height of the abdomen. Through this, the pelvic diameters are increased to the maximum, the anterior shoulder due to the straightening of the sacrum and the movement of the posterior shoulder over the sacrum descends below the pubic symphysis and the posterior shoulder descends lower into the pelvis36-38. However, McRoberts’ is not always successful. In case of traction of the head there is high risk of complications such as brachial plexus injury of the newborn (BPI)37,39. Moreover, lower extremity neuropathy due to prolonged compression of the femoral nerve of the mother and complications such as hip stiffness and extension of the knee to the site of injury could occur36.
Suprapubic pressur
McRoberts’ is often combined with suprapubic pressure18,19,35,38,39 where a second health-worker applies pressure with a palm or fist down and sideways to move the anterior shoulder below the pubic symphysis and towards the oblique diameter of the pelvis, which is the largest diameter. It is recommended in cases of mild shoulder dystocia18,35. Interestingly, the American College of Obstetricians and Gynecologists’ current recommendation is to begin with this maneuver combined with suprapubic pressure. In fact, the success of the aforementioned combination ranges 24–62%34.
Jacquemier’s maneuver
This maneuver consists of delivery of the whole posterior arm followed by posterior shoulder delivery40; it is recommended when the McRoberts maneuver combined with suprapubic pressure fails and it is not a primary maneuver18,35. In general, because of the difficulty of the maneuvers and the pain to the woman, an epidural anesthesia is mandatory. The obstetrician inserts a hand into the vagina behind the posterior fetal shoulder to grasp the fetal elbow and bend it to the fetal chest. Then, with gentle traction, the fetal elbow is delivered followed by the delivery of the posterior shoulder. If this fails, it is recommended to rotate the fetus internally so that the anterior shoulder is now posterior and then repeated. However, this has been related to complications such as humerus fracture, especially when flexion of the elbow is impossible or difficult17,18,35.
Wide episiotomy
Wide episiotomy is necessary to be performed to facilitate the procedures7,19,41-43. More specifically, the maneuver of Rubin–Wood needs more space in order to be efficient7,12,19,35,37,39,42. This procedure is included in most algorithms such as the Hernandez & Wendel and the ALARMER and, placed as an obligatory procedure before the internal maneuvers, except in the HELPERR algorithm7,9. In summary, the majority of authors recommend to perform a wide episiotomy.
Gaskin maneuver (‘all-fours’ position)
This maneuver is inspired from the traditional procedures of dystocic deliveries in Guatemala. The mother is placed in a knee-hands position7,27,35,37 or in a sprinter position35,41 but never in a knee-chest position7,35. In this way the cavity of the sacrum increases and the gravity in combination with the traction of the posterior or anterior shoulder facilitates the release of the shoulder27,35. However, this treatment is not indicated in cases of epidural or dorsal anesthesia7,35.
Second-line maneuvers
Posterior axillary traction
Posterior axillary traction is recommended as a second internal maneuver if the delivery of the posterior shoulder fails18,35,41 which, according to Ansell et al.17, appears to have better results and is thus recommended to be used as the first internal maneuver if McRoberts’ with suprapubic pressure fails37. The health worker places a hand into the posterior aspect of the pelvis and with the thumb and first finger grasps the posterior shoulder around the axilla, and with the middle finger applies traction only through the axilla. As a result, the posterior shoulder is delivered followed by the delivery of the anterior arm18,35,37.
Rubin maneuver
The Rubin maneuver (rotation of the shoulder) was first described in 196434. It involves rotating the shoulders to the oblique diameter through suprapubic pressure7,35,37. If this fails, Rubin II is recommended. The physician inserts a hand into the vagina after anesthesia and applies pressure to the anterior aspect of the most accessible shoulder in order to reduce the bisacromial diameter7,27 then rotates the shoulder27,35,37. Clinical studies have shown that the Rubin maneuver is associated with fewer complications and requires less traction compared to the McRoberts maneuver7,35. However, it is more invasive than the McRoberts maneuver and less easily performed in patients without anesthesia35.
Wood’s maneuver
Wood’s maneuver (rotation of the fetus) is the second internal maneuver after Rubin’s and these two are quite often combined7,35,37. It was first described in 194234. This maneuver puts pressure on the front clavicle surface of the posterior shoulder so that the fetus rotates 180 degrees and the front shoulder is released35,37. If combined with the Rubin maneuver then pressure is applied to both shoulders clockwise or counter clockwise to rotate the baby7,35.
Third-line maneuvers
Intentional clavicular fracture
This is achieved by applying pressure to the clavicle of the fetus, when more conservative approaches fail7,27. This technique reduces the bisacromial diameter, but the clinician must be very careful so not to injure the underlying vascular fracture or even the lung fracture27,35.
Zavanelli maneuver
When all techniques have failed, then the Zavanelli maneuver is suggested2,19,37. This maneuver came into popular use in the early 1980s. The mother receives terboutaline sc or some other uterine relaxant7,35. The fetal head should then be turned in the anterior occipital position, flexed from the extended position and then pushed back into the pelvis. A cesarean section is performed immediately7,27,35,37. During the procedure it is mandatory to monitor the fetal heart rate35.
Symphysiotomy
Symphysiotomy is only recommended when all other techniques have failed7,27,35,37. In fact, Menticoclou18 states that it should be applied only after 5 minutes if the dystocia has not been solved yet and the other maneuvers, even the Zavanelli, have failed. It has been used as a last resort. It involves the surgical division of the fibrous tissue and cartilage7 of the pubic symphysis7,35,37 in order to increase the pelvic diameters7,35. However, it should be avoided because the separation of the pubic symphysis is not restored and has been related to complications such as bladder, urethral and vaginal injury. These injuries could lead later to urinary incontinence, chronic pelvic pain, and unstable pelvis7,35,37.
Algorithms
Although Gottlieb and Galan6 consider that there is no specific algorithm for the management of shoulder dystocia, most researchers suggest various algorithms.
The HELPERR
The HELPERR7,25 algorithm is as follows: Help, Evaluate (for episiotomy), Legs (McRoberts’ position), Pressure (suprapubic), Enter (rotational maneuvers), Remove (posterior arm), and Roll (hands and knees).
The Hernandez & Wendel
The Hernandez & Wendel algorithm involves: 1) Call for help, 2) Wide perineotomy, 3) Suprapubic pressure, 4) McRoberts’ maneuver, 5) Delivery of the posterior arm, and 6) Wood’s screw maneuver or Rubin maneuver.
The ALARMER
The ALARMER algorithm when the episiotomy in contrast to HELPERR is in 6th place7.
The British and French College
The British College of Obstetricians and Gynecologists and the Collège National des Gynécologues et Obstétriciens Français2 propose the following algorithm: 1) Call for help, 2) No pushing, 3) McRoberts’ maneuver, 4) Suprapubic pressure and gentle head traction, 5) Wide perineotomy, 6) Jacquemier’s maneuver and Rubin’s or Wood’s maneuver, and if there is a failure, 7) Knee-elbow position, and repeat algorithm. If this also fails then the third-line maneuvers: clavicle fracture, Zavanelli maneuver, and symphysiotomy, are recommended7,37.
Prevention
It is notable that cesarean section should be recommended in order to prevent shoulder dystocia only in the following cases: 1) fetus with weight >4.5 kg, if associated with maternal diabetes; 2) fetus with weight >5 kg and with an absence of maternal diabetes; 3) previous history of shoulder dystocia with severe maternal and neonatal complications; and 4) fetal macrosomia with a failure in progress to the second stage of delivery2. The main point is knowledge of the weight of the fetus, to avoid a difficult delivery including shoulder dystocia. This could be assessed by ultrasound which can estimate approximatively the weight of the fetus, but in some cases it can be over- or under-estimated. In case of very probable macrosomia, a cesarean section should be performed in order to avoid the difficult delivery of shoulder dystocia.
CONCLUSION
Shoulder dystocia is an unpredictable obstetrics emergency and many maneuvers have been proposed for its management. The key to successful management is anticipation and suitable preparation. For this reason, both obstetricians and midwives should be able to perform all the obstetrics maneuvers and as quickly as needed in order to prevent potentially serious consequences. There is a need for an experienced team in this situation, on the other hand the maneuvers should be performed without losing time because each minute is crucial to avoid severe complications or death of the fetus.