

INTRODUCTION
The latent phase of labor is characterized by irregular uterine contractions and gradual cervical changes and may last several hours or even days1-3. Although it represents a normal physiological stage of childbirth, its definition and management vary considerably across clinical guidelines and care settings3. While some guidelines define the onset of active labor at 4 cm cervical dilation, others recommend waiting until 5 cm or 6 cm, leading to inconsistencies in admission practices and clinical decision-making1-4.
Women often seek hospital admission during the latent phase, due to pain, uncertainty, or anxiety, and the need for reassurance5-11. However, early admission has been associated with higher rates of obstetric interventions, including augmentation and cesarean section11,12. Consequently, many guidelines recommend delaying hospital admission until active labor is established, provided that maternal and fetal conditions are reassuring11. Despite these recommendations, in clinical practice, the management of latent labor remains challenging. Midwives must balance institutional policies, resource constraints, medico-legal considerations, and women’s individual needs. In systems with limited outpatient structures, counseling women to return home during the latent phase could be particularly difficult.
In Germany, maternity care is predominantly hospital-based and has been shaped by increasing centralization and ongoing workforce shortages13. In addition to salaried hospital-employed midwives, some maternity units collaborate with self-employed midwives (‘freelance midwives’) who work under independent contractual arrangements and are remunerated on a case-by-case basis through statutory health insurance. These midwives often provide intrapartum care within hospital settings but are not directly employed by the hospital. As a result, their scope of practice and remuneration structures differ from those of salaried staff. In summary, the current financial and organizational frameworks provide only limited support for outpatient care during the latent phase of labour14,15. Together, these structural conditions may influence admission decisions and shape midwives’ scope of practice. Although several international studies have examined women’s experiences during the latent phase, less is known about midwives’ perspectives on providing care under these structural constraints, particularly within the German healthcare system. Understanding midwives’ experiences is essential for identifying barriers and potential strategies to improve care during latent labor. Therefore, this study aims to explore midwives’ perspectives on resources and challenges when supporting women during the latent phase of labor within the German maternity care system (Table 1).
METHODS
Design
A qualitative study employing expert interviews was conducted to explore professionals’ perspectives on care during the latent phase of labor. A semi-structured interview guide with open-ended questions enabled adaptive probing to capture emerging themes16. All participants provided written informed consent. In accordance with GDPR requirements, interview recordings and anonymized transcripts were stored on researchers’ secure, password-protected laptops.
Sampling and selection of participants
In Germany, midwives are the primary care providers for physiological births. In 2024, 98% of the 680017 births occurred in a clinical setting. A purposive theoretical sampling strategy was used to capture variation in organizational contexts of maternity care. Participation from midwives working across different levels of perinatal care was intentionally sought, as well as different institutional sizes and urban/rural settings, to explore how structural conditions may shape care during the latent phase of labor. The aim was to interview ten to fifteen midwives who work in an obstetric setting. Midwives who worked in a clinic for at least 50% of their weekly working hours for at least six months were included. To investigate correlations between care capacity for the latent phase and clinic location and size factors, participants were categorized according to their hospital’s perinatal care level. It should be noted that as a result of the 2024 hospital reform, the designation of the care levels changed17. During the interviews, the former classification of care levels was used. Participants were recruited via an invitation flyer, which was distributed by email, letter, or in person to maternity wards in the federal states of Lower Saxony, Schleswig-Holstein, Hamburg, and Bremen.
Data collection
The interview guide was developed by two midwives based on exploratory literature research and refined in a workshop with experienced researchers. Its relevance and clarity were pre-tested by Mother Hood e.V., a parents’ organization advocating for improved obstetric care in Germany. The questions addressed care resources for women in the latent phase, diagnostic and decision-making criteria, counseling content, and professional perspectives on optimal care. Interviews were conducted face-to-face or by telephone by an experienced midwife researcher. Audio recordings were transcribed verbatim18, anonymized, and linguistically refined for readability19. Transcripts were returned to participants for validation. Quotations used in the manuscript were translated into English, with original quotations and translations presented in Table 2.
Table 2
Illustrative quotations from interviews with midwives on care during the latent phase of labor (English translation and original German)
Analysis
The evaluation employed qualitative content analysis following the approach proposed by Kuckartz et al.19, using the MaxQDA 2022© software. As part of the preliminary textual analysis, the anonymized transcripts were reviewed in accordance with the dual control principle, and key topics were identified. These were then summarized and categorized. For further processing, the preliminary results were presented at a research colloquium. A category system was then developed inductively, resulting in four main categories and twelve subcategories. As practicing midwives, the authors were aware of their own professional perspectives and discussed potential biases during analysis.
Ethical considerations
Ethical approval was granted by the Ethics Committee of Carl von Ossietzky University Oldenburg (file number 2024-049). The study is reported in accordance with the SRQR checklist20. All participants received written information about the study and provided informed consent. Participation was voluntary, and confidentiality was ensured throughout the research process.
RESULTS
In the period between 17 June 2024 and 3 March 2025, thirteen midwives were interviewed in person or via telephone. The interviews lasted between 28 and 65 minutes. Twelve midwives were employed or were freelancers (self-employed) at a hospital in Germany. One midwife specialized in out-of-hospital obstetrics and, following her own concept, provided outpatient care during the latent phase. She was therefore included in the sample to provide an expert perspective on care during the latent phase. Table 3 provides a comprehensive overview of the sample.
Table 3
Characteristics of participating midwives and workplace settings, qualitative interview study conducted in Germany, 2024–2025 (N=13)
Four main categories were identified: 1) physiology of the latent phase, 2) decision-making regarding location of care, 3) structural hospital conditions, and 4) care improvement. Table 4 presents the category system with anchor quotes.
Table 4
Category system derived from qualitative content analysis, including definitions and anchor quotations, based on interviews with midwives in Germany, 2024–2025 (N=13)
The physiology of the latent phase
Definition
Midwives described differing criteria for identifying the onset of labor, and emphasized the relevance of women’s subjective perceptions when determining support needs. Many considered the latent phase to be part of the birthing process, rather than a separate preliminary stage:
‘... I find that difficult because some women are already stressed at 1.5 cm and need support. ... they might not be in labor, but they still need care.’ (I8)
A few midwives expressed uncertainty about defining the latent phase as strictly physiological, particularly when distress or a prolonged duration occurred. A uniform professional definition was perceived as lacking.
Facilitating factors
Midwives identified both physical and psychological factors that may promote physiological progression of the latent phase. Commonly mentioned were relaxation measures (e.g. baths, TENS, movement) and continuous emotional support. Encouraging women to view the latent phase as a meaningful part of birth was considered beneficial.
Inhibiting factors
Midwives identified subjective and structural factors that may hinder progression, including invasive interventions, exhaustion, misinterpretation of support needs, and language barriers:
‘... I think it depends on how well informed they [women] are about it in advance. So, if they somehow know ... and have come to terms with the fact that it can take a long time, then it’s okay for them. The men tend to be more nervous than the women. But yes, of course, some are impatient or just exhausted and stressed at some point. And maybe that’s what happens, that they [midwives] just want to help somehow because the women are there [in the hospital], after all.’ (I2)
Overall, midwives described the latent phase as a sensitive transition requiring individualized support, where unmet informational or emotional needs may increase stress.
Decision-making criteria for the location of care
Once the diagnosis has been made, the woman, her birth companions, and the obstetric staff decide on various criteria regarding where the latent phase should be spent. Differences in assessment emerged regarding the balance between medical criteria, personal preferences, and institutional constraints.
Medical history
Midwives assessed parameters such as parity, complications, rupture of membranes, and travel distance when considering admission. Medico-legal concerns were frequently mentioned, and sometimes led to precautionary admissions:
‘Yes, legal concerns always play a role ... Even if a woman calls with contractions, you tend to ask her to come in because you have to check ... simply so no one can say that she called and then something was wrong with the baby afterward ...’ (I8)
Such defensive practices were described as barriers to needs-based care and were sources of stress.
Safety and pain perception
Women’s desire for security and pain relief often influenced admission decisions:
‘... you can filter out those who are actually doing well ... and those that are just not comfortable at home anymore. Those are the ones who are clearly in need of support, and that support might just mean hearing the baby once, getting an exam, and being told that this is still the early stage of labor.’ (I5)
Midwives noted that the individual sense of safety frequently outweighed clinical criteria. While supporting this need, they acknowledged that limited resources restricted individualized counseling or observation. Overall, the decisions made reflected tensions between guidelines, institutional frameworks, and women’s expectations, requiring midwives to balance professional responsibility and autonomy.
Structural conditions in the hospital
Care capacities and infrastructure
Midwives emphasized that the quality of care largely depended on staff availability and spatial resources. Limited space and understaffing often constrained individualized care. Some midwives mentioned that financial incentives could influence the timing of admission, especially in self-employed settings:
‘... we are a team of freelancers. If we are being honest, we don’t earn money from the birth itself, but rather from providing care as early as possible, or rather, from providing care for a long time beforehand. And that tends to lead to women being called in relatively early ...’ (I5)
Monitoring and birth management
After admission, fetal and maternal parameters were regularly monitored. Participants described a pressure for timely obstetric progress and a variability in tolerance for prolonged latent phases across settings:
‘... we also have one or two colleagues who come from other clinics, who would tolerate the cervix being three or four centimeters dilated for a long time without anything being done. I wasn’t familiar with that at all. So really, she [colleague] is saying, “Yeah, she was four centimeters dilated for three hours.” And in principle, that’s fine. It’s just the latent phase; that’s allowed to happen. Of course, you always have to see how the woman is doing, but three years ago, I wouldn’t have had that. After two hours at the latest, something would have happened; we would have given her the drip [oxytocin] or broken her waters [amniotic sac]. So, there would have already been some sort of intervention to get things moving ...’ (I1)
Midwives described frustration when prolonged, painful latent phases occurred without progress, while supportive, continuous care was structurally limited:
‘It’s a difficult phase when women can’t cope ... Because there is nothing worse than 24 hours of painful contractions with no progress ... And that is my secret frustration when I hear the term “latent phase”.’ (I6)
Overall, participants perceive structural and financial constraints as major barriers to individualized, womancentered care. Limited space and staffing, and institutional expectations sometimes lead to early admissions and interventions, even when midwives prefer a more conservative approach.
Aspects for care improvement
The midwives who participated in the survey set out various ideas and suggestions for improving the quality of care during the latent phase.
Support and counseling concepts
Midwives proposed strengthening midwife-led outpatient models, including telephone assessment and home visits, as well as designated hospital rooms for women in the latent phase:
‘So, I think to myself: Let’s do it the way the WHO recommends, meaning midwife-led facilities for assessing the onset of labor and the latent phase, upstream of the delivery room. ... With appropriate documentation, with appropriate facilities, in case people don’t want to tackle an extremely long drive, but want to be at the place of birth. That we just make sure that they can use everything that promotes the latent phase.’ (I3)
‘I think it would help many women if their midwives ... could accompany them at home during the latent phase ... so that this latent phase could somehow also be covered for women outside the hospital. Where they don’t yet enter this cascade of interventions in the delivery room, in the hospital, and into this expectation, so to speak, and still feel safe and secure. I think some women ... need this sense of security ...’ (I13)
Restructuring resources
Participants recommended improved remuneration for on-call duties and reduced insurance costs for outpatient midwives. They also advocated for more staff and appropriate spaces, noting that low-risk pregnancies do not necessarily require high-level facilities:
‘A completely normal pregnancy doesn’t actually require a Level 1 facility ... You could say: these women can just stay in a kind of latent phase room and then have their baby there. They don’t need all the big machinery. I think this would also free up resources for latent-phase care ...’ (I8)
Further training and education of specialist staff
Participants called for additional professional education about the latent phase and better communication skills, particularly in English, to improve counseling for diverse patient groups:
‘Yes, and unfortunately, many of the midwives don’t speak English either. I would like to see a general training requirement. All colleagues should at least learn the basics so that they can communicate with all women. Or they should consistently use [translation app for mobile phones] ... and not just ignore the woman and take it easy on the job.’ (I12)
To avoid unnecessary interventions, they also saw a need to raise awareness among doctors about the physiological nature of the latent phase:
‘If doctors are informed about what the latent phase is, what women need during this time, and what it’s all about, then I think that would be fine. I don’t think we’ve yet optimized how to support women ... But I wouldn’t say that there is a one-size-fits-all solution. You always have to weigh the pros and cons, and unfortunately, I don’t have a magic fix that helps everyone (laughs), and neither do the doctors; they are often unsure themselves ...’ (I6)
Prenatal information and education
Midwives emphasized prenatal education as a key factor for coping with the latent phase. To promote realistic expectations and self-efficacy among women and their birth companions, they suggested addressing the topic in antenatal classes, early counseling, and even school-based education:
‘... preparing the person accompanying the birth, because they also have immense potential to influence the timing of care, out of uncertainty. That’s why it’s so important to look at these resources and also to make sure that this information about the physiology of the latent phase is really part of the preparation, that this accompanying person is prepared ...’ (I3)
Participants also suggested more detailed registration consultations, although time constraints and limited reimbursement often restricted such approaches. Overall, midwives expressed a strong desire for structures that enable continuous, needs-based care in hospital and outpatient settings, highlighting training, prenatal education, and systemic reforms as key strategies.
DISCUSSION
This study shows that in Germany, access to needs-based care during the latent phase of labor remains limited. Midwives reported frequent early admissions when they perceived increased support needs, despite guidelines recommending inpatient admission only at the onset of active labor. A central concern was the lack of structured outpatient options: women sent home often receive no professional support, as few midwives provide home-based latent-phase care, partly due to financial disincentives and liability concerns14. These findings should be interpreted in light of the dual structure of German midwifery employment models, in which salaried hospital-employed midwives work alongside self-employed midwives providing care under independent contractual arrangements. This organizational context may shape both continuity of care and financial incentives during the latent phase.
Midwives described the latent phase as a professional and ethical dilemma. They viewed themselves as advocates for women’s needs, while being constrained by institutional routines and legal frameworks. Diverging definitions of the onset of labor – whether the latent phase is considered part of labor or a preliminary stage – shaped admission practices. These findings align with previous research showing a limited consensus on diagnostic criteria1-3 and similar structural challenges in latent labor management in other high-income countries6,21.
Participants highlighted supportive measures such as rest, reassurance, and movement as potentially facilitating physiological progress, although effects vary individually. The blurred boundary between supportive and medical interventions, combined with managing exhaustion or distress in a phase defined as physiological, often limited the perceived care options. Similar uncertainties and counseling demands have been reported elsewhere6,8. Differences also emerged between clinical assessments and women’s subjective needs, with many women prioritizing safety, which is often associated with hospital monitoring6,8. Admission decisions were further influenced by contextual factors, including parity, travel distance, language barriers, and medico-legal concerns. Increasing distances to maternity units following hospital closures may reinforce precautionary admissions, as travel time becomes an additional safety consideration.
Structural and financial conditions were described as major determinants of care quality. Adequate staffing and space were considered prerequisites for personalized support, while high workloads and limited infrastructure restricted counseling and individualized management. Financial incentives shaped practice in different ways: in some settings, early care provision was economically advantageous, whereas in others, remuneration decreased when caring for several women simultaneously22,23. Such inconsistencies may inadvertently promote early admission and intervention cascades. Although participants were recruited from facilities with different levels of perinatal care, no clear pattern of attitudes towards latent-phase management emerged according to care level alone. Rather, midwives across settings consistently described staffing levels, workload, and the number of women requiring simultaneous care as key factors shaping admission decisions and the ability to provide individualized support. Given the small and heterogeneous sample, these observations should be interpreted cautiously.
Participants proposed strengthening midwife-led outpatient models, including telephone assessments, home visits, or designated latent-phase rooms within hospitals. International examples, such as Ireland’s Labor Hopscotch Framework24, indicate that structured, low-intervention environments may improve resource allocation and women’s experiences. However, sustainable financing and clear liability coverage were regarded as essential prerequisites for implementation in Germany. Antenatal education was identified as another key strategy. Early, realistic information about the latent phase – provided in classes, consultations, or registration interviews – may reduce anxiety and unnecessary early hospital attendance. Yet such counseling is frequently underfunded and inconsistently reimbursed25.
Midwives also called for professional training to strengthen the understanding of the latent phase among both midwives and doctors. Improved knowledge of its physiology could reduce pressure for interventions and support shared decision-making. Language skills were additionally regarded as essential for equitable care in increasingly diverse patient populations.
Overall, the findings illustrate how structural, professional, and emotional factors intersect in shaping care during the latent phase. Systemic reforms – ensuring adequate staffing, appropriate facilities, fair remuneration, and clear liability frameworks – appear to be central to improving woman-centered care. Integrating midwife-led continuity concepts and strengthening antenatal education should enhance autonomy and satisfaction while reducing unnecessary interventions. Future research should evaluate the implementation and outcomes of innovative latent-phase care concepts, ideally through co-design approaches involving women, midwives, and policy makers26.
Although this study is situated in the German healthcare system, similar challenges regarding latent labor management, use of resources, and midwife-led concepts have been described across international settings7-11. The findings, therefore, contribute to ongoing discussions about strengthening midwife autonomy and the continuity of care within maternity systems.
Strengths and limitations
This study is the first to explore midwives’ perspectives on caring for women during the latent phase of labor in Germany. The main strength of this study lies in its exploration of a largely unexamined area of maternity care. The inductively developed category system can inform further research and guide policy discussions on how to strengthen midwife-led, woman-centered support during the latent phase. While it provides valuable insights into professional experiences and structural barriers, several limitations must be acknowledged. As the study focused exclusively on midwives working within the German healthcare system and was conducted in German, transferability to other countries is limited due to differing legal, financial, and organizational frameworks for midwifery care.
The qualitative design involved a small, non-representative sample of thirteen midwives. The findings, therefore, reflect subjective viewpoints and cannot be generalized to all midwives or clinical settings. The sample size also did not allow meaningful comparisons between participants working in different levels of perinatal care. However, the aim of qualitative research is to gain an in-depth understanding, rather than statistical representativeness27, and the sample was purposefully diverse in terms of professional background and institutional context. Nevertheless, the uneven distribution of participants across different perinatal care levels limits the ability to compare hospital types, with midwives from high-risk facilities being underrepresented. Despite these constraints, participants provided detailed accounts of their working environments and identified potential links between structural conditions and care quality.
Implications
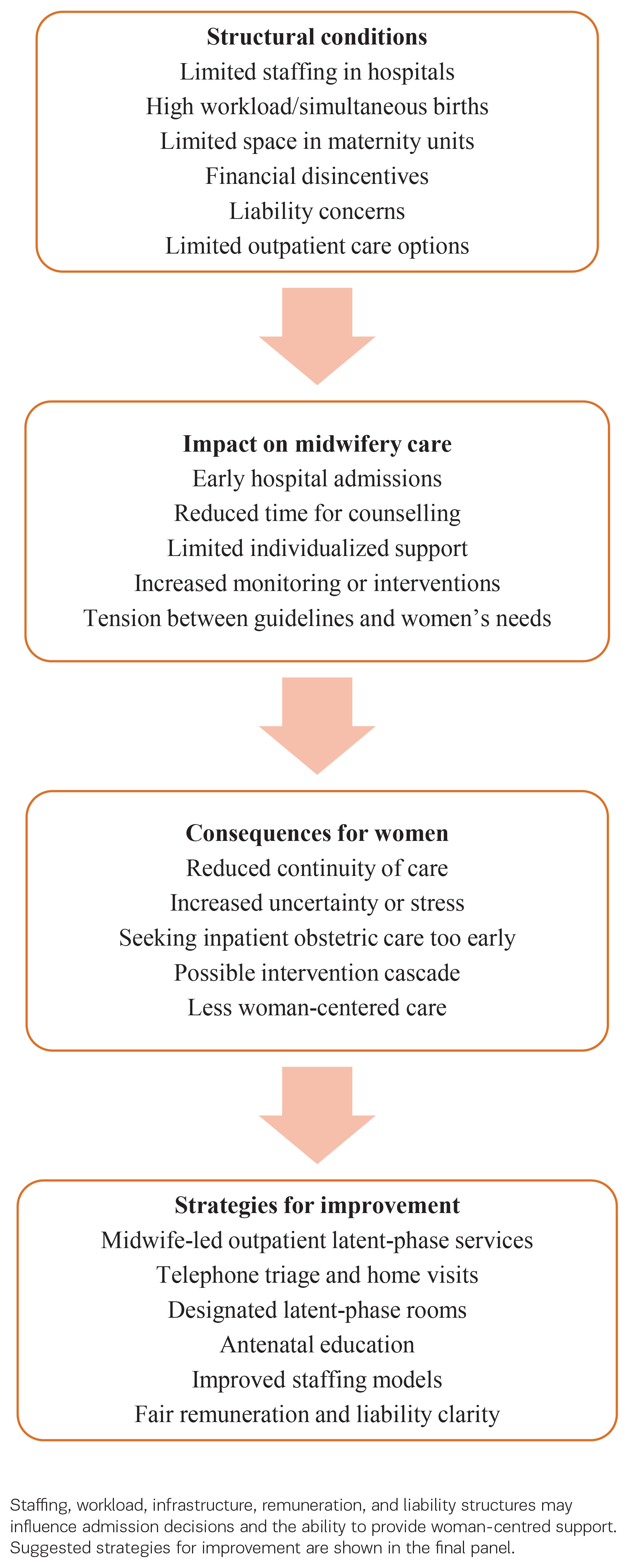
Midwives should be enabled and supported in providing guidance and continuity of care during the latent phase of labor across community and hospital settings. Strengthening midwife-led outpatient care, antenatal education, and designated latent-phase spaces within maternity units could reduce unnecessary interventions, improve access to appropriate care during the latent phase, and promote woman-centered care. Sustainable remuneration models and clear liability frameworks are essential to make such approaches feasible in routine practice. Practical priorities include piloting midwife-led outpatient latent-phase services, integrating preparation for the latent phase into antenatal education, ensuring staffing models that allow sufficient time for counseling and individualized support, expanding equitable access to latent-phase care, and improving access to translation resources for women with limited proficiency. Further research should examine the feasibility, acceptability, and outcomes of these approaches, while policymakers should adapt reimbursement structures to better support continuity of care and clearly define midwifery roles during the early stage of labor. The structural factors influencing care during the latent phase of labor and potential strategies for improvement are illustrated in Figure 1.
CONCLUSIONS
This qualitative study identified key resources and barriers shaping midwives’ counseling and care during the latent phase of labor in Germany. The findings indicate that structural and financial conditions strongly influence both admission decisions and the quality of woman-centered support. Staffing levels, workload, and spatial limitations were described as major factors determining whether midwives could provide individualized care. Self-employed midwives working in hospitals also face financial disincentives that may restrict their ability to offer comprehensive latent-phase support.
These challenges highlight the need for structural reforms to ensure fair remuneration, clear liability frameworks, and sustainable staffing models. Midwives expressed strong interest in innovative, midwife-led approaches – such as outpatient counseling, home visits, and designated latent-phase rooms within hospitals – that could align women’s needs for safety and continuity with professional and institutional realities. Enhanced prenatal education and well-resourced registration consultations may also help reduce unnecessary early admissions.
Future initiatives should evaluate the feasibility and outcomes of co-designed care models within the German context. Strengthening midwife-led continuity of care and expanding outpatient counseling options could improve women’s experiences during the latent phase, reduce intervention rates, and contribute to a more balanced and sustainable maternity care system. Additional training for obstetric staff on managing the latent phase could further enhance the quality of care.
Reorganizing latent-phase care is not merely a clinical issue, but a structural and policy challenge. Supporting midwives in providing continuous, needs-based care during latent labor will represent a key step towards more sustainable and woman-centered maternity services in Europe.