

INTRODUCTION
Labor pain is a complex and multifaceted element of childbearing women’s experiences1. Pain is defined as an intense and unpleasant sensory experience, associated with contractions that the woman would like to avoid or alleviate2. The difference between pain and suffering is key in supporting laboring women’s physical and emotional wellbeing. Suffering is a distressing psychological state that includes feelings of helplessness, fear, panic, loss of control, and loneliness2. Simkin et al.3 suggest midwives should focus on the ability of woman to cope with pain, rather than the pain itself. Coping is defined as the person’s cognitive and behavioral efforts meant to manage challenging or stressful situations. Non-pharmacological coping strategies such as postural changes, breathing techniques, vocalization and relaxation, could be powerful resources in the management of intrapartum anxiety and pain4.
NICE guidelines5 recommend to consider the woman’s emotional and psychological needs and to observe how women deal with pain and manage it. WHO guidance6 advises healthcare providers to consider relaxation techniques for pain management, such as muscle relaxation, massage, application of warm packs, breathing, music, mindfulness and other techniques, depending on the woman’s preferences. Laboring women’s ability to cope with pain is likely to be dependent on a variety of inter-related factors, including the level of pain intensity, the nature of the environment and the perceived support6.
Previous research on coping strategies mainly focused on these individually7-10, with international guidance partially covering them5,11 and a systematic literature evidence synthesis of these not being available. The aim of this systematic review was therefore to explore coping strategies used by laboring women, related outcomes and factors influencing coping with labor pain.
METHODS
Design and literature search strategy
A mixed-methods systematic review was undertaken. Electronic databases (Medline, EMBASE, CINAHL, PsycInfo) were searched to identify eligible studies from December 2020 to November 2021, published in English or Italian. Search terms included: ‘wom*n’, ‘pain’, ‘lab*r’, ‘coping’, and ‘strategies’. Synonyms and MeSH terms were identified and included in the search strategy. Keywords were combined using Boolean AND and OR in search strings; truncation was used when required.
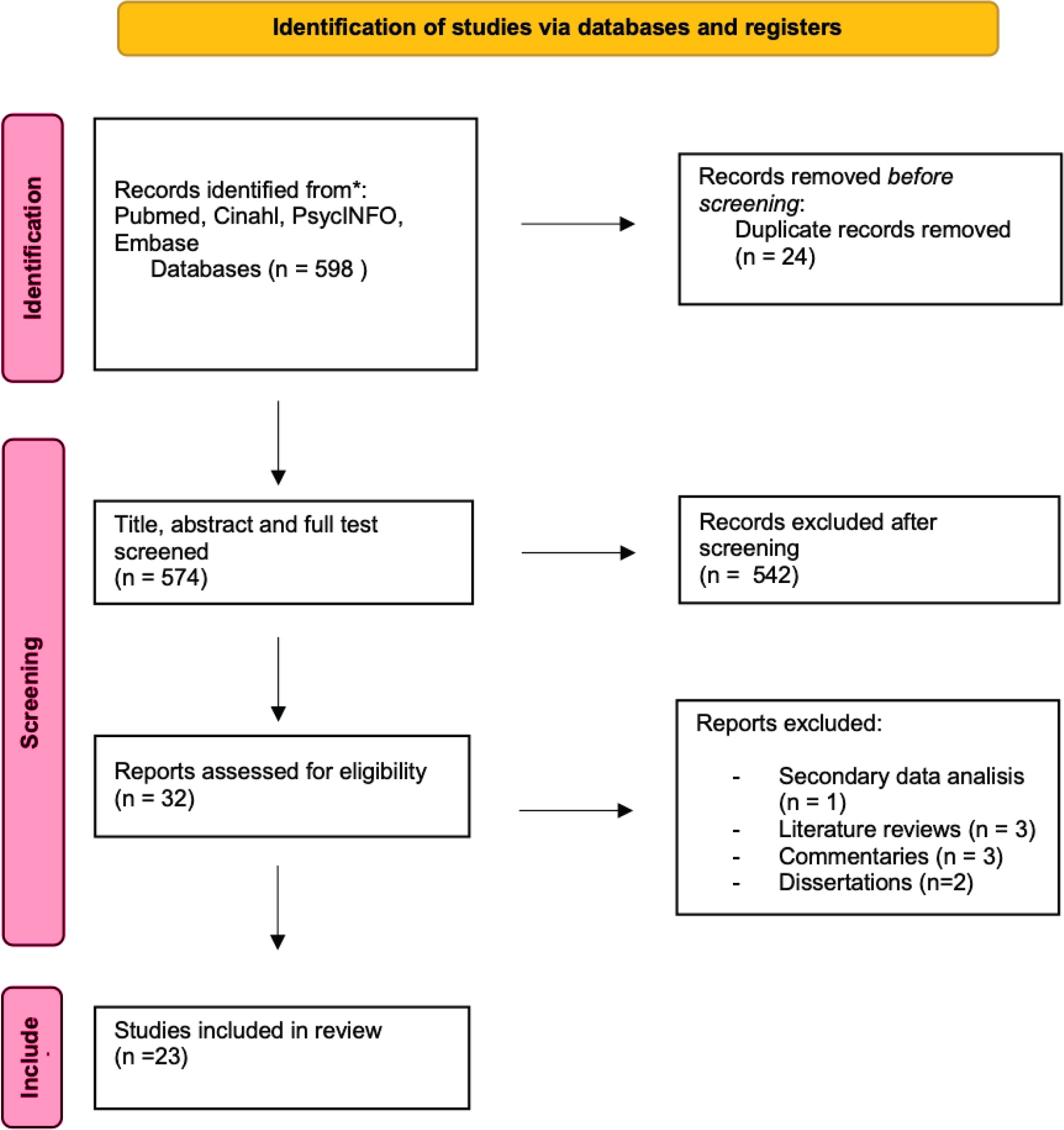
Articles were included in the review if they met the following criteria: English or Italian language; systematic reviews, quantitative or qualitative primary research studies; published up to November 2021; focus on labor coping strategies and related influencing factors. Exclusion criteria were: secondary data analysis, literature reviews and commentaries; focus on coping strategies with pain other than labor pain. We conducted the search and reported the findings according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines12. The literature search and inclusion process are detailed in the PRISMA flow diagram12 in Figure 1. All references retrieved during the systematic search were stored in EndNote. After removal of duplicates, titles and abstracts were initially screened for eligibility. Articles whose abstracts alluded to the search topic were selected for full-text screening and if relevant, data were extracted and recorded for inclusion in this review. The reference lists of relevant studies were searched manually to identify additional relevant articles, and their full texts screened to ensure that all potentially useful articles were included. A list of articles meeting the inclusion criteria was compiled. Two authors independently evaluated the studies’ fulfillment of the inclusion criteria, with any discrepancy discussed with a third author until a final set of relevant studies was agreed upon.
Quality assessment
The quality of studies included in the review was evaluated using a range of established critical appraisal tools selected for the study design and Joanna Briggs Institute13 levels of evidence: Critical Appraisal Skills Programme14 tools for qualitative, cohort and case control studies; STROBE check-list for observational studies15; and MMAT QA tool16 for mixed-methods studies. Two independent researchers assessed the quality of the selected articles and banded studies as low, medium or high quality, with consensus achieved. Although no studies were excluded on the basis of quality, the quality assessment was used to critically consider the strengths and limitations of the evidence retrieved17.
Data abstraction and synthesis
Data abstraction forms were independently completed by two researchers. Qualitative findings were interpreted and organized into themes and sub-themes following a thematic analysis approach18. The quantitative findings were narratively synthesized and reported thematically19. The final mixed-methods synthesis involved gathering qualitative and quantitative data and producing a set of synthesized findings.
Findings
Twenty-three studies were included. These were conducted between February 1985 and March 2021 in the United Kingdom (n=9), Iran (n=2), Netherlands (n=2), USA (n=3) and other countries (n=7). The quantitative articles (n=15) included 4 randomized controlled trials, 5 correlational studies, and 6 observational studies. There were 2 mixed-methods studies and 6 qualitative studies. The following data were extracted from the included studies: general information (authors, publication year, country of investigation), population (number of participants), study design, key findings and outcomes (Table 1).
Table 1
Characteristics of studies involved in the systematic review
| Authors Year Country | Title | Number of participants | Study design | Key findings and outcomes |
|---|---|---|---|---|
| Spiby et al.7 2003 United Kingdom | Selected coping strategies in labor: An investigation of women’s experiences | 121 women, who had self-selected for attendance at antenatal classes | An exploratory research design | The effects of the coping strategies investigated varied widely among participants. Common aspects of care, changes of environment, and use of pharmacological pain relief affected women’s discontinuation of coping strategies. |
| Bergstrom et al.8 2010 USA | How caregivers manage pain and distress in second-stage labor | 23 laboring women of low-to-moderate obstetric risk | Secondary qualitative analysis of data (videotapes) from the Second Stage Labor Project. They used linguistic and conversational analysis methods to produce microanalytic descriptions of interaction patterns of talk and observational methods to describe their efficacy. | They identify patterns of behavior used by laboring women and describe successful and unsuccessful strategies used by caregivers to help women deal with pain and distress during the second stage of labor. |
| Slade et al.9 2000 United Kingdom | Antenatal predictors and use of coping strategies in labor | 121 primiparous mothers | Correlational study | When coping strategies were used, they were generally continued for substantial proportions of time. Greater proportions of use of breathing and relaxation were associated with labor being experienced as less frightening. High proportions of women believed that using coping strategies would be associated with benefits in particular enabling feeling more positive, calm and in control and reducing pain in labor. Women were less likely to believe that use of coping strategies would lead to reductions in use of analgesia. |
| Fadhil et al.10 2021 Iraq | Assessment of potential factors that affect women response to labor pain at Al-Elwyia maternity teaching hospital | 60 laboring women | A descriptive quantitative study | A significant positive relationship was found between labor stress and pain, and from environmental factors in primiparas and in multipara women in study made in 2009. |
| Beebe et al.20 2007 USA | The effects of childbirth selfefficacy and anxiety during pregnancy on prehospitalization labor | 35 English-speaking nulliparous women, with uncomplicated pregnancies | A longitudinal, descriptive study | Prenatal anxiety was significantly related to self-efficacy for childbirth in late pregnancy, labor pain, number of hours at home in labor, and admitting cervical dilation. The number of management strategies used was related to pain scores during labor before hospital admission. |
| Abushaikha et al.21 2007 Jordan | Methods of coping with labor pain used by Jordanian women | 100 Jordanian low-risk women who had normal vaginal deliveries | A combination of quantitative (descriptive statistics) and qualitative (content analysis) components | This study confirms previous findings regarding coping methods and adds new knowledge on coping with labor pain among Jordanian parturients. The significance of childbirth education as a means to inform Jordanian women about coping with labor pain is emphasized. |
| Escott et al.4 2004 United Kingdom | The range of coping strategies women use to manage pain and anxiety prior to and during first experience of labor | 43 primiparous mothers | Qualitative semi-structured interviews | The findings indicate that it is possible to help women during pregnancy to identify and describe, in their own words, the range of coping strategies used to manage previous experiences of pain and anxiety. In addition, they provide understanding of the coping strategies used during labor by women who had not attended antenatal classes. |
| Niven et al.24 1996 United Kingdom | Coping with labor pain | 51 women | An exploratory research design | The results of this study indicate that a considerable range of coping strategies was used by women during childbirth. Many of these seemed, in essence, similar to those considered in the empirical literature and resembled strategies that women had used previously. The total number of strategies used in labor was negatively correlated with levels of labor pain, suggesting that the use of coping strategies in labor can modulate the pain. |
| Asl et al.25 2018 Iran | Relationship between behavioral indices of pain during labor pain with pain intensity and duration of delivery | 120 low risk pregnant women | Cross-sectional study | Behaviors demonstrated by women in labor had effects on their pains in the course of delivery, and there was also a relationship between the duration of stages of labor and severity of pain. |
| Shiloh et al.26 1998 Israel | Interactive effects of viewing a contraction monitor and information-seeking style on reported childbirth pain | 48 low risk women giving birth in a hospital near Tel Aviv | Within-subjects experimental design | Monitored women experienced less pain‚ and blunted more pain while viewing the monitor‚ controlling for contraction amplitudes. Women viewing the monitor used more attention and control-predictability strategies than when not viewing‚ particularly if they had a monitoring information-seeking style; when not viewing the monitor they used more distraction strategies‚ particularly if they had a blunting information-seeking style. Reported use of attention‚ distraction‚ and control-predictability coping strategies had significant negative correlations with pain reports. Pain anxiety was positively‚ and self-efficacy expectations negatively‚ related to pain reports. |
| Klompt et al.27 2017 Netherlands | A qualitative interview study into experiences of management of labor pain among women in midwife-led care in the Netherlands | 17 women | Qualitative interview study | Women reported that control over decision making during labor (about dealing with pain) helped them to deal with labor pain, as did continuous midwife support at home and in hospital, and effective childbirth preparation. Some of these women implicitly or explicitly indicated that midwives should know which method of pain management they need during labor and arrange this in good time. |
| Leap et al.28 2010 United Kingdom | Journey to confidence: Women’s experiences of pain in labor and relational continuity of carer | 10 women who reflected on their experiences of preparation and support for pain in labor and midwifery continuity of carer with Albany midwives | A qualitative descriptive methodological approach | Women reflected positively on how, throughout pregnancy and labor, their midwives promoted a sense of their ability to cope with the challenge of labor pain. These experiences enhanced women’s ability to overcome fears and self-doubt about coping with pain and led to feelings of pride, elation, and empowerment after birth. |
| van Haaren-Ten Haken et al.29 2018 Netherlands | Birth place preferences and women’s expectations and experiences regarding duration and pain of labor | 454 nulliparous women | A prospective cohort study | Women who preferred a home birth were significantly less likely to expect difficulties with coping with pain and were significantly less likely to experience labor pain as unpleasant. |
| Thies-Lagergren et al.30 2021 Sweden | Being in charge in an encounter with extremes. A survey study on how women experience and work with labor pain in a Nordic home birth setting | 1649 women with a planned homebirth | Mixed method | While labor pain was often experienced as positive or very positive, the intensity was experienced as severe or the worst imaginable pain. Two main themes arose from the women’s descriptions of their birth experience regarding labor pain: An encounter with extremes and being in charge at home. |
| Fathi Najafi et al. 31 2017 Iran | The best encouraging persons in labor: A content analysis of Iranian mothers’ experiences of labor support | A total of 25 women, including 16 women in labor and having the experience of a natural childbirth, two women who had recently given birth, one birth companion, one doula midwife, two midwives, one obstetrician, one resident in obstetrics, and one medical student, were finally selected | An exploratory qualitative study | Three categories, including ‘involvement of the spouse in the labor process’, ‘asking for a companion during labor’, and ‘mother’s self-care to cope with labor pain’, emerged during data analysis. These categories were merged to form the main theme of ‘trying to comply with the labor process’. |
| Campbell et al.32 2019 United Kingdom | ‘It definitely made a difference’: A grounded theory study of yoga for pregnancy and women’s self-efficacy for labor | 22 women attending yoga for pregnancy classes | A longitudinal grounded theory study | Yoga for pregnancy enhances women’s self-efficacy for labor by building their confidence and competence through a combination of techniques. |
| Ip et al.33 2009 China | An educational intervention to improve women’s ability to cope with childbirth | 133 Chinese first-time pregnant women | Randomized controlled trial | The educational intervention based on Bandura’s self-efficacy theory is effective in promoting pregnant women’s self-efficacy for childbirth and reducing their perceived pain and anxiety in the first two stages of labor. |
| Copstick et al.34 1985 United Kingdom | A test of a common assumption regarding the use of antenatal training during labor | 60 primiparous mothers | An observational study | Mothers who used both breathing and postural techniques dropped out significantly as labor progressed, less than a third of all the mothers using any coping techniques at all by the beginning of the second stage of labor. Of the more than two-thirds remaining, a substantial number can be accounted for by them having had epidural analgesia, though some of the epidural mothers did continue to use their coping techniques. However, this still leaves over half of the ‘non-epidural’ mothers not using any coping techniques at all by the second stage of labor. |
| Leventhal et al.35 1989 USA | Active coping reduces reports of pain from childbirth | 89 normal pregnant women in two separate studies. Because of procedural problems in Study 2, the final samples consisted of 48 participants in the first study, while the replication used a sample of 29 | Experimental design | In Study 1 (N=48) pain and negative moods showed a sharp decline at Stage 2 (active labor) for women told to monitor and those who had attended classes; there was no decline for the control group. In Study 2 (N=29), women attending Lamaze classes reported a similar decline in pain during active labor and were more energetic and less tired at admission. |
| Guder et al.36 2019 Cyprus | The effect of childbirth preparation training on primiparous women’s birth plans and the childbirth processes | 70 primiparous women | A quasi-experimental/non-randomized trials and prospective study | Midwives and nurses play an active role in the realization of the birth plans that are within the framework of prenatal education courses. The experimental group had a lower rate of planned cesarean, were more satisfied with their childbirth experiences, received more support during the birthing process, and used more techniques for coping with pain during labor. |
| Naidu et al.37 2020 India | A study to assess the effect of childbirth education on intrapartum coping behaviors of primiparous women in a selected maternity center of a tertiary level hospital in Pune | 60 registered primigravidae attending the ANC OPD of a hospital at Pune | A prospective quasi-experimental study | Primigravidae were poorly informed about childbirth preparedness and not prepared for the experience of childbirth. Majority had no concept regarding the severity of pain, duration of labor and coping measures stress of labor. Significant reduction in episiotomy rates, use of analgesics and improvement in coping behaviors found among the experimental group. |
| Escott et al.38 2005 United Kingdom | Preliminary evaluation of a coping strategy enhancement method of preparation for labor | 20 women participated in antenatal classes incorporating the CSE method and 21 women participated in antenatal classes incorporating the standard approach to developing coping strategies for labor | Randomized controlled trial | Women who attended CSE classes used enhanced coping strategies for a larger proportion of their labor than women who attended standard classes who used taught coping strategies. Birth companions were more involved in women’s use of enhanced than taught strategies. Self-efficacy for use of coping strategies and subsequent experiences of pain and emotions during labor were equivalent between groups. |
| Spiby et al.39 1999 United Kingdom | Strategies for coping with labor: does antenatal education translate into practice? | 121 primiparous women | An exploratory within-subjects research design | The findings of this study of a group of well-prepared women raise questions about the correct components of antenatal classes and how midwives and birth companions can be involved optimally in this aspect of a woman’s labor. |
Three themes were identified: 1) definition of coping and types of coping strategies, including behavioral and cognitive based techniques; 2) coping strategies related outcomes, including improvements in self-efficacy and reduction of pain intensity, fear, anxiety, time of admission and labor duration; and 3) factors influencing coping with labor pain, including continuity of carer, environment, presence of a birth companion, cardiotocography monitoring, and antenatal education. Themes and sub-themes are summarized in Table 2. Behavioral and cognitive coping methods, factors influencing coping with labor pain and sources from where these were reported are included in Table 3.
Table 2
Themes and sub-themes
Table 3
Behavioral and cognitive coping methods, factors influencing coping reported by studies involved in the systematic review
| Studies | Behavioral coping strategies | Cognitive coping strategies | Influencing factors | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Breathing technique | Maternal postures | Use of hands (holding, pressure) | Vocalizing | Distraction | Attention | Focusing on pain | Imagination | Relaxation | Spirituality | Continuity of carer | Environment | Birth companion | Cardiotocography monitoring | Antenatal education | |
| Spiby et al.7 | ✓ | ✓ | ✓ | ||||||||||||
| Bergstrom et al.8 | ✓ | ✓ | |||||||||||||
| Slade et al.9 | ✓ | ✓ | ✓ | ||||||||||||
| Fadhil et al.10 | ✓ | ✓ | ✓ | ✓ | |||||||||||
| Beebe et al.20 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||||
| Abushaikha et al.21 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||||||
| Escott et al.4 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||||
| Niven et al.24 | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||||||
| Asl et al.25 | ✓ | ✓ | ✓ | ||||||||||||
| Shiloh et al.26 | ✓ | ✓ | |||||||||||||
| Klompt et al.27 | ✓ | ✓ | |||||||||||||
| Leap et al.28 | ✓ | ||||||||||||||
| Van Haaren et al.29 | ✓ | ||||||||||||||
| Thies-Lagergren et al.30 | ✓ | ||||||||||||||
| Fathi Najafi et al.31 | ✓ | ||||||||||||||
| Campbell et al.32 | ✓ | ||||||||||||||
| Ip et al.33 | ✓ | ||||||||||||||
| Copstick et al.34 | ✓ | ||||||||||||||
| Leventhal et al.35 | ✓ | ||||||||||||||
| Güder et al.36 | ✓ | ||||||||||||||
| Naidu et al.37 | ✓ | ||||||||||||||
| Escott et al.38 | ✓ | ||||||||||||||
| Spiby et al.39 | ✓ | ||||||||||||||
Theme 1: Definition of coping and types of coping strategies
The first theme identified related to the definition of coping and to the range of coping strategies women adopt to stay with pain during labor.
Amongst the 22 selected articles, only three4,20,21 provided a definition of coping. Two articles4,20 refer to the definition given by Lazarus and Folkman3, describing coping as the person’s cognitive and behavioral efforts aimed at handling challenging or stressful situations, intended as an on-going individual adjustment process in order to be effective.
One article21 reports two definitions of coping from Beutler and Moos22 and from Brown and Nicassio23. The first definition refers to coping as a complex and multidimensional phenomenon with cognitive, emotional and behavioral qualities, leading to changes and adaptation22. The second one explains coping as particular thoughts and behaviors adopted to stay with the pain or with the emotions generated from the pain23.
Women use a variety of coping strategies for managing labor pain, including behavioral and cognitive based techniques21. Behavioral strategies are defined by Beebe et al.20 as ‘those activities that participants mentioned physically doing’; whereas cognitive strategies referred to ‘those things they were thinking about that were associated with managing their labor’.
Nine articles4,7-10,20,21,24,25 included a range of behavioral coping strategies used by women to deal with labor pain and four techniques were identified: breathing, maternal positions, holding/pressure, and use of voice.
Breathing was the most used by women, in particular the ‘slow, deep breath’ techniques are the most cited methods4,7-10,21,24,25. One source mentioned the ‘slow sigh’ strategy9 and another one the ‘blow’ as breathing techniques24. A variety of movements and maternal positions were adopted by laboring women, including walking, rocking, swaying4,7,9,10,20,21,24, squatting9,21, all fours, one side, sitting, and upright4. Additional methods reported by women to manage labor pain are the use of hands for holding something or for applying pressure4,10,20,21. The use of voice was mentioned by five articles4,8,20,21,25 including vocalization, singing, and murmuring. One article cited also the method of counting numbers during contractions8.
Eight sources4,7,9,20,21,24-26 included a variety of cognitive coping strategies used by women to manage labor pain and seven techniques were identified: distractions, attention, imagination, focusing on pain, relaxation, and spirituality.
Three articles4,21,24 mentioned using distraction as a cognitive coping strategy frequently used by women, meaning the need to take the mind off their pain, such as counting numbers4 or thinking about future events such as the imminent birth of their baby21. Attention was proposed by one study26 as a mechanism that laboring women adopt to stay with the pain. Women with limited mobility during labor, looked at the contractions on the cardiotocography monitor as a method to get away from the pain stimulus.
Imagination was found in two sources21,24 as a technique that women used to think of a different place rather than the birthplace, or a way to visualize their baby’s body and face24, or the exact moment of birth21.
Three articles4,21,24 described focalization on labor pain as helpful for laboring women. Of these, one22 reported that women focused on thinking of a positive purpose for the pain, that pain is limited over time, and how other women before them experienced and coped during that time. In addition, women tried to prepare themselves for each contraction during labor, being aware that although very painful they would be able to manage them21.
Amongst the three selected articles7,9,25 that considered relaxation techniques as very important strategies to deal with labor pain, none reported what they intended specifically with this term. One article21 cited spiritual coping methods such as praying, reading holy books, having confidence in God, and trying to find a scope and a meaning for pain.
Theme 2: Coping strategies related outcomes
A decrease in the overall average level of labor pain24 and lower pain scores during labor at home20 were observed in women who adopted more coping strategies. Amongst behavioral coping strategies, Slade et al.9 report that women using breathing techniques rated pain as less severe. Women who used more behavioral coping strategies stayed home longer in the early labor phase20. Childbearing women’s self-efficacy related to the number of management strategies adopted, rather than the type of techniques used20. Breathing and relaxation techniques were associated with labor being experienced as less frightening9. The use of cognitive coping strategies lowered women’s levels of anxiety (measured by the Spielberger State-Trait Anxiety Inventory scale)20. Behavioral indicators (e.g. face expressions, verbal expressions, tone of voice, body movements, relaxation and breathing patterns) during labor were significantly and inversely associated with the duration of the active phase of the first stage of labor and the duration of the second stage of labor25. An increased average score of behavioral indicators during labor reduced the overall duration of the first and second stage of labor25. Behavioral indicators were significantly and inversely correlated with the perceived intensity of labor pain25.
Theme 3: Factors influencing coping with labor pain
The factors influencing coping with labor pain identified within the selected articles are: continuity of carer, environment, presence of a birth companion, cardiotocography monitoring, and antenatal education.
The continuity of carer facilitated by caseload models enabled the establishment of a trusting relationship and good communication between the woman and midwife, impacting positively on the woman’s self-efficacy and active involvement in the decision-making process in regard to pain relief strategies, therefore improving the ability to cope with pain27,28.
A positive coping experience seemed to be facilitated by the woman laboring in an environment of her choice in accordance to individual needs and preferences29,30.
The presence of a birth companion played a key role within the woman’s ability to cope with pain, mainly through the use of verbal and non-verbal encouragement, calming approach and physical touch22,31.
Cardiotocography may have beneficial effects on coping with pain due to laboring women implementing control and predictability strategies when looking at the monitor26. The use of cardiotocography did not seem to impact on breathing and relaxation techniques, but limited the laboring woman’s positions and movement7.
A number of articles present the positive impact of different types of antenatal education on the woman’s ability to cope with labor pain and to use a variety of coping strategies27,32-37, mainly due to: increased self-efficacy27,32-34; more accurate perception of childbirth; improvement of perceived safety; reduced pre-labor distress; and encouragement of positive feelings in regard to labor and birth35. When women were encouraged to think about a birth plan as part of antenatal education, it was more likely they would apply coping strategies in labor resulting in increased pain control27,36. The effectiveness of different antenatal education approaches may be dependent on an individual woman’s needs38. Spiby et al.39 report that some women found the coping strategies taught during antenatal education classes unsatisfactory, with <5% of women feeling extremely competent in implementing each strategy. Antenatal classes were less effective in regard to more advanced labor stages and especially during the second stage of labor, due to the increased difficulty in applying coping skills34.
DISCUSSION
This systematic review explored coping strategies used by laboring women, related outcomes, and factors influencing coping with labor pain. The findings of our systematic review identified a variety of behavioral and cognitive coping strategies and recognized increased benefits when women adopted these during labor, including improvements in self-efficacy and reduction of pain intensity, fear, anxiety, time of admission and labor duration. The combination of several strategies, rather than the type of techniques used, particularly improved women’s self-efficacy, highlighting the multidimensional and complex nature of labor pain1. The promotion and use of non-pharmacological pain relief coping strategies is recommended by WHO11 as part of respectful and supportive maternity care. Fetal and neonatal outcomes in relation to the use of coping strategies in labor were not reported by any of the selected article. In regard to maternal outcomes, emotional wellbeing was mainly explored within the retrieved sources, with only few clinical outcomes investigated (pain intensity, time of admission, and labor duration). Our findings identified antenatal and intrapartum factors influencing coping with labor pain, including antenatal education, continuity of carer, environment, birth companion, and cardiotocography. The impact of antenatal education on coping has been widely explored within the selected articles, highlighting the key role of information provision during pregnancy and prior to labor40 to improve maternal satisfaction with the childbearing event41,42. Borrelli et al.43 recommended midwives should dedicate time to discuss with women and birth partners what coping strategies or pain relief they have been considering, ideally during the second or third trimester of pregnancy. Limited evidence was found on the other influencing factors mentioned above. Despite that only two of the selected articles described the presence of a birth companion as key within the woman’s ability to cope with pain4,31, it is broadly acknowledged that birth partners play a significant role with the woman’s overall childbearing experience and satisfaction44. The same applies to continuity of carer27,28, with the consistency of a known midwife or small team of midwives being recognized as crucial to the successful design and delivery of maternity care services45. The maternal choice of birthplace is encouraged5,6 to support women’s individual needs and self-efficacy in coping with pain.
Strengths and limitations
The strengths of the review included the use of a rigorous and systematic methodology to define, classify and synthesize the best available evidence on the topic under investigation, covering a knowledge gap. In addition, data can be transferable to similar settings at international level. The review included articles only published in English, which represents a limitation of the review, as relevant studies reported in other languages may have been excluded.
CONCLUSIONS
This systematic review provides midwives and healthcare professionals with information to recognize coping strategies spontaneously adopted by laboring women and promote the use of a variety of techniques, as required by individual needs and preferences. Midwives are also provided with up-to-date knowledge on coping strategies related outcomes and influencing factors, which they can utilize to guide evidence-based practice decision-making and facilitate women’s and families’ informed choice. Further research should focus on a more comprehensive investigation of maternal, fetal and neonatal clinical outcomes and influencing factors to assess the short/ medium/long-term effectiveness of coping strategies.